
The ampule of digoxin was accidentally taken from automated dispensing cabinet instead of bupivacaine
The ampule of digoxin was accidentally taken from automated dispensing cabinet instead of bupivacaine

Prefilled diluent and vaccine syringes may be easily mixed up

Specifying a day of the week to take the medication could help avoid inadvertent daily dosing

Although the brand name manufacturer updated the label after the FDA’s request, generic manufacturers have not all followed suit.

Incorporate Program Requirements Into Systems and Workflows.

Because the generic name of both the timolol once-daily and twice-daily formulations is the same, pharmacies should only carry 1 formulation.

Inaccurate information, miscommunication during transition points can have dire consequences.

Errors risk transmission of blood-borne pathogens, including HBV, HCV, HIV, to health care providers, patients.
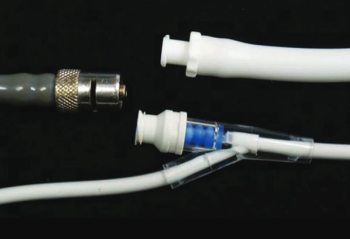
Death occurs from air embolism after pneumatic line was connected to an intravenous catheter.

Establish procedures, including training employees, to address shortages, back-order situations.

Clinical decision support, packaging changes can help stop errors related to the HIV medication.

Learn strategies to safeguard use of the intravenous administration products to protect patients.

Protect patients by evaluating VIGIV concentration and avoiding tearing of metal flange on vaccine vial.

Pharmacists should engage patients, explore system fixes to prevent missed drug-drug interactions

Specialty pharmacy reports case of alirocumab prescription with mg incorrectly typed instead of mL.

Take steps to safeguard prescribing, dispensing, and patient use of the COVID-19 antiviral medication.
Resources for health care professionals include FDA’s patient eligibility screening checklist tool for prescribers.

Mark these products for mandatory patient education on the cartons and in the pharmacy computer system.

Case highlights the need to stop, listen, and investigate when patients or parents express a safety concern.

Expediting the dispensing process makes sense, but take care when entering and verifying script.

Although the ISMP created the guidelines for hospitals, they are applicable in other health care settings.

Implementation, communication, and assessment are critical steps to ensure patient safety.

Institute for safe medication practices receives hundreds of reports of incorrect doses for children.

Pharmacies should address situations in which multiple bottles of tablets are used to refill a cassette.

Clonidine, Estradiol, Fentanyl, and Scopolamine are involved most frequently, an ISMP review shows.

Discontinued fentanyl infusion left attached to patient contributes to his death, but risk-reduction strategies can prevent similar mistakes.
Pharmacists should provide both verbal education and written instructions, so mistakes do not occur.

It is time to standardize to a single formulation to avoid mix-ups that can lead to adverse effects.

Companies and practitioners should take important steps to protect patients from these mistakes.

When patients report pharmacy errors, respond with empathy and transparency to avoid alienating them.
Published: August 19th 2022 | Updated:

Published: September 26th 2022 | Updated:
Published: March 24th 2011 | Updated:
Published: July 5th 2011 | Updated:
Published: April 18th 2013 | Updated:
Published: May 17th 2013 | Updated: